Most NCDs do not have a cure. Networking among multidisciplinary teams that could have the training and capacity to face disease from a perspective of causative pathomechanisms, such as NRF2 related dysfunction, rather than “only” the specific clinical symptoms, is the most appropriate approach to overcome this drawback. Therefore, the challenge of BenBedPhar is to share NRF2-related knowledge generated by evidence-based pharmacological and clinical research, and to integrate it into the stream of European social, clinical and economic sectors with capacity to translate this knowledge into innovative therapeutics for a set of NCDs. Obviously, not all NCDs will benefit equally from NRF2-related therapy and the Action will define the most suitable ones. However, overwhelming evidence supports a focus on: metabolic [diabetes, nonalcoholic steatohepatitis (NASH)], cardiovascular, neurodegenerative disease, and at least two types of cancer (lung cancer where over 30% have KEAP1/NRF2 mutations, and glioblastoma where NRF2 is activated by signaling mechanisms.
On the other hand, several parapharmaceutical companies have jumped into this field and are marketing natural NRF2 modulators, often originating from herbal traditional medicine. Not at all questioning the important value of natural products for drug discovery, these compounds are propagated as alternatives to school medicine and magic bullets against various diseases without evidence for bioavailability, efficacy, quality control or risk assessment. While this fact demonstrates the increasing public interest in NRF2-therapy, BenBedPhar will raise awareness about the current limitations of NRF2-related compounds and their use without clinical proof of efficacy or safety.
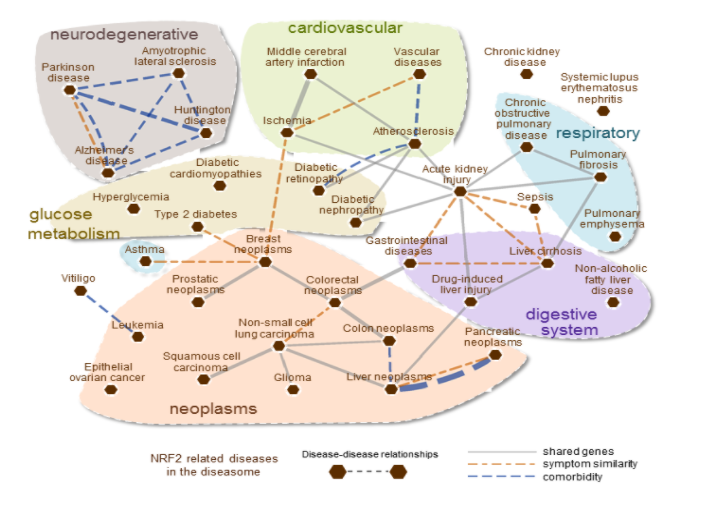
The NRF2 diseasome. The relationships between diseases are represented as a network in which pathophenotypes are linked by common genetic and clinical descriptors. In the figure, nodes (red hexagons) represent diseases, and the edges are similarities among them based on shared genes, common symptoms, and comorbidities (gray, orange, and blue lines, respectively). The genes and symptoms associated with the diseases are used to identify disease pairs that have a significant genetic and symptomatic overlap calculated using the Jaccard index. Among significant disease–disease connections (P < 0.05, assessed by Fisher’s exact test based on the observed gene or symptom overlap), only the links that have an elevated overlap and comorbidity are shown to eliminate potentially spurious connections. Accordingly, the diseases that share at least 10% of the disease-associated genes and more than half of the associated symptoms are included in the figure. The comorbidity information is extracted from medical insurance claims, representing disease pairs that tend to occur together in the population (relative risk >2) (source, Cuadrado et al. Pharmacol Rev. 2018 Apr;70(2):348-383).